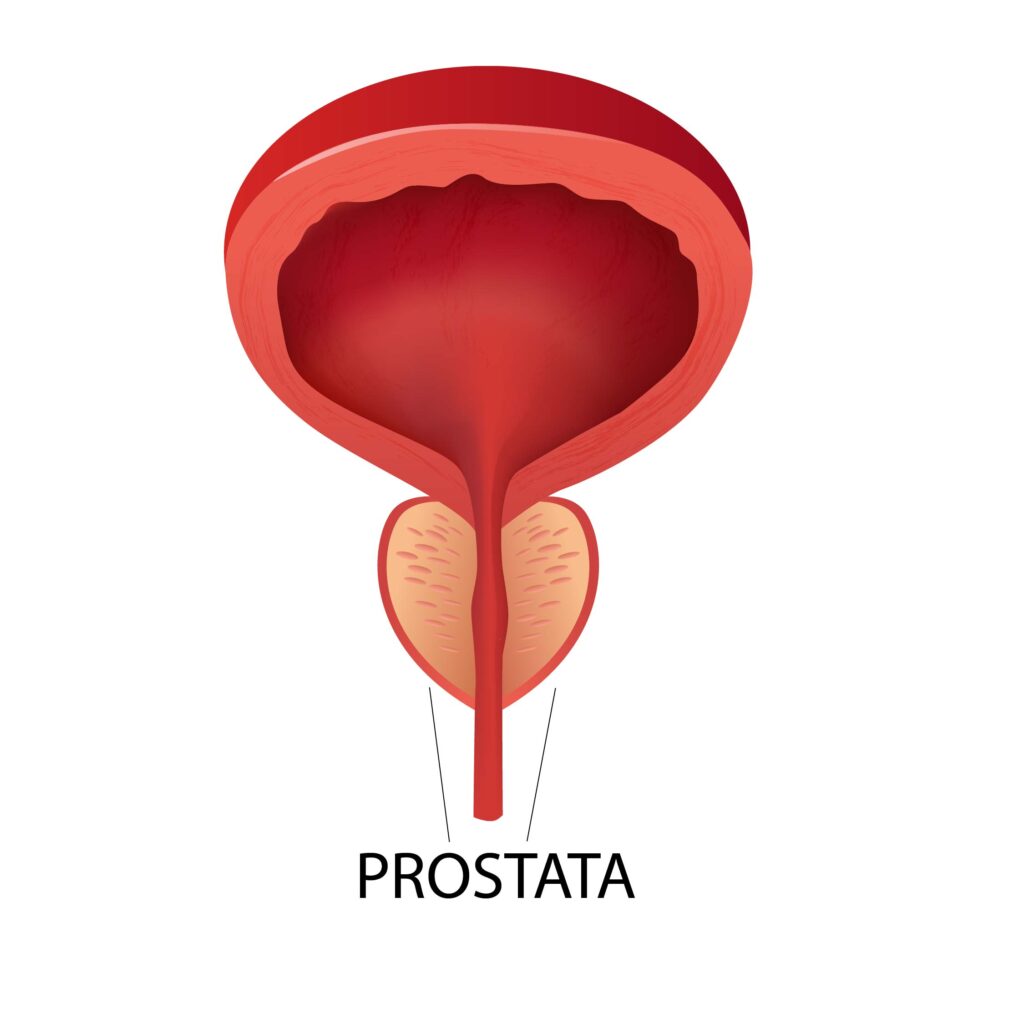
What is the Prostate?
The prostate is an exocrine gland specific to men, located below the bladder, surrounding the upper part of the urethra. Its main role is to secrete an alkaline fluid that forms an important part of the seminal fluid, contributing to the survival and mobility of sperm cells.
Main Functions:
- Production of Prostatic Fluid: The prostate secretes an alkaline fluid that makes up approximately 30% of the total volume of semen. This fluid protects and nourishes sperm, facilitating their mobility and survival in the acidic environment of the female reproductive tract.
- Contribution to Fertility: Prostatic fluid contains essential enzymes and proteins that maintain the fluidity of semen and optimize conditions for fertilization.
- Regulation of urinary flow: By surrounding the urethra, the prostate also plays a role in controlling urinary flow. Prostate conditions can lead to compression of the urethra as it passes through the prostatic urethra, causing difficulties in urination.
What is Prostate Adenoma?
Prostate adenoma is the enlargement of the gland due to the proliferation of glandular tissue, a phenomenon that generally occurs after the age of 50, with the frequency of this condition increasing with advancing age. The enlargement of the prostate (its hypertrophy) takes place under hormonal influence, as prostatic tissue becomes more sensitive to the action of testosterone after a certain age. Prostate adenoma is a slowly progressing condition, developing over several years, with the changes it induces on the urinary system appearing insidiously.
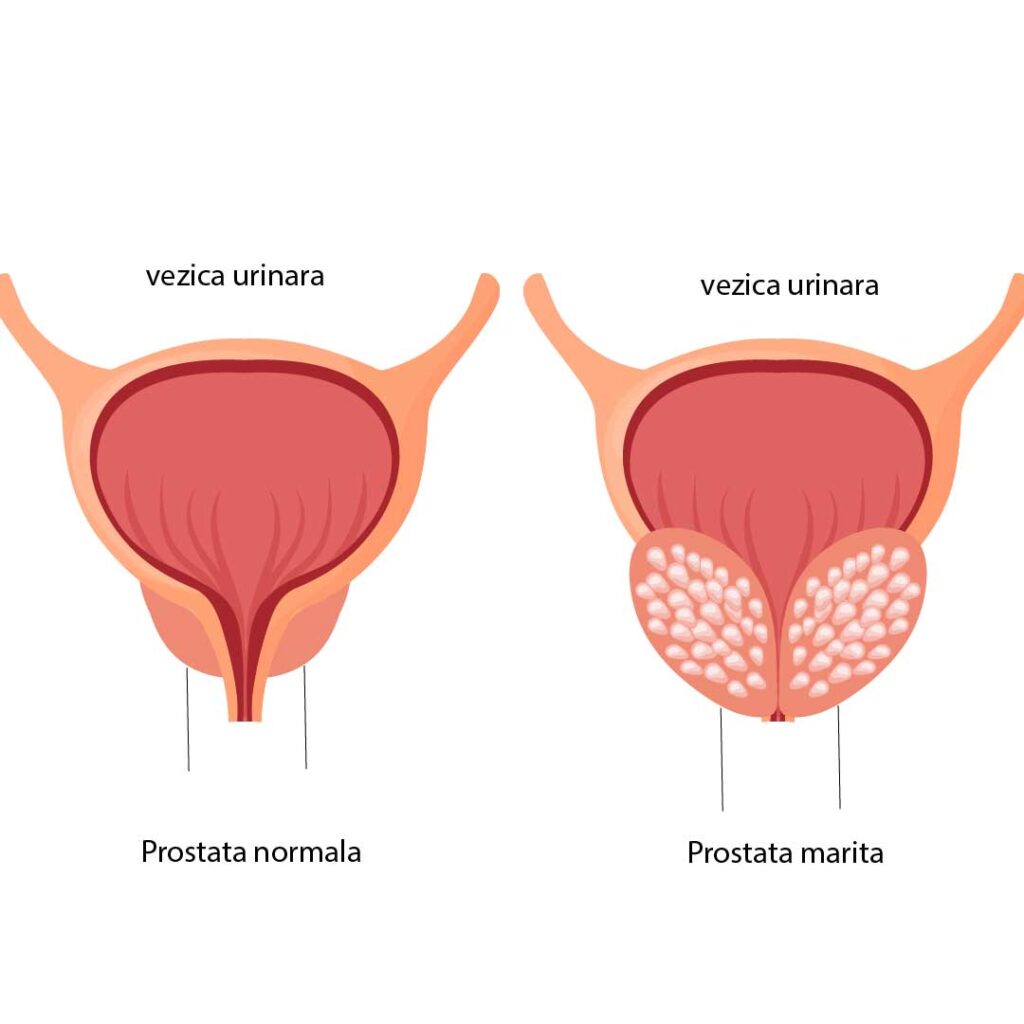
Prostate enlargement (development of prostate adenoma) gradually compresses the urethral caliber, causing changes in both urinary and reproductive function. For proper emptying of the bladder, when the prostate adenoma obstructs the normal elimination of urine, the bladder muscles and abdominal muscles attempt to overcome this obstacle through additional effort, so that initially the urinary stream and flow are not affected. Later, even if these muscles contract more strongly, this mechanism becomes insufficient, leading to the so-called “battle bladder,” in which the bladder walls become hypertrophied and thickened. The incomplete emptying of the bladder explains the appearance of “residual urine,” meaning the remaining amount of urine left inside the bladder after urination, this phenomenon being responsible for the complications of prostate ade
The increase in prostate size in prostate adenoma means that, from a volume of 15–25 cm³ in a young or middle-aged man, the prostate can reach 40, 50, or even 100 cm³ (sometimes more).
The risk factors implicated in the development of prostate adenoma are: genetic factors, age, alcohol consumption, smoking, high blood pressure, obesity and diabetes mellitus, as well as the use of certain medications (antidepressants, antihistamines).
Symptoms
OBSTRUCTIVE SYMPTOMS
Difficulty in initiating urination, weak urine stream, intermittent or interrupted stream, difficult urination, prolonged bladder emptying time, feeling of incomplete bladder emptying, loss of urinary control, feeling of incomplete bladder emptying, urinary retention (“urine blockage”).
IRRITATIVE SYMPTOMS
Increased frequency of urination (pollakiuria), especially at night (nocturia), urgency (the sudden and compelling urge to urinate), urge incontinence (the man 'leaks' a few drops before reaching the toilet).
Diagnosis
The diagnosis of prostate adenoma and its possible complications is made only by a specialist urologist, following a clinical examination and the paraclinical investigations recommended by the doctor and performed by the patient.
Investigations for Prostate Adenoma
1. Detailed medical history
The urologist will ask you about your medical history, especially your urological history: the symptoms you are experiencing, their severity, and how they affect your daily life. You will also be asked about the quality of your erections, since poor erections can be caused by obstructive prostate symptoms. Some medications may affect bladder function, and it is important for the doctor to rule out those medications. In younger men (under 45 years), symptoms similar to those caused by prostate obstruction are often due to conditions such as urethral stricture (narrowing of the urethra) or prostate inflammation (acute or chronic prostatitis). The urologist will therefore ask about any history of trauma, conditions, or surgeries involving the urethra that may lead to the development of strictures.
2. Physical examination
You will undergo a complete physical examination, including blood pressure measurement. The doctor will perform a digital rectal examination to assess the size and consistency of the prostate. Abdominal examination may also be useful to reveal a possible enlargement of the bladder.
3. Laboratory tests
- Complete blood count, renal function tests (blood urea and creatinine) - PSA level – usually measured from the blood of men with obstructive symptoms; if the PSA level is higher than normal or if the prostate appears altered on digital rectal examination, the urologist will recommend additional tests to rule out prostate cancer. An elevated PSA level does not mean the presence of prostate cancer. 50–60% of men with prostatic hypertrophy have increased PSA levels. The only way to rule out prostate cancer is a consultation with a urologist to recommend further investigations; - Urinalysis – a urine sample will be sent to the laboratory to rule out a possible urinary tract infection.
4. Other specific tests
An abdominal X-ray may be indicated, as well as an abdominal ultrasound to evaluate prostate volume and post-void residual urine, and uroflowmetry (assessment of urinary stream pressure).
TREATMENT
When medication therapy no longer provides the expected results, meaning the patient begins to experience recurrent urinary tract infections, or bladder stones develop, or ultrasound shows that the bladder is no longer emptying completely, or even acute retention or urinary blockage occurs, surgical treatment options become necessary.
When a man experiences one of the symptoms of prostate adenoma, there are several options regarding the treatment of this condition:
Medication Treatment
It represents a first option in the treatment of prostate adenoma. This method is effective in patients with mild to moderate symptoms and is limited over time, as the medication can provide beneficial effects for a period of up to 10–15 years.
Alpha-blockers are the first type of medication prescribed by the urologist. They relax the muscles inside the prostate and the bladder neck, facilitating the passage of urine. They may cause side effects such as low blood pressure, difficult or absent ejaculation, and nasal congestion.
5-alpha reductase inhibitors: They reduce the volume of the prostate gland (recommended for prostates larger than 50 cm³) and can be used together with alpha-blockers if the PSA level is higher than 1.5 ng/ml (a possible indicator that the prostate is significantly enlarged). These medications may cause erectile or libido problems. The effect of 5-alpha reductase inhibitors is noticeable after 6 months of treatment. They also reduce PSA levels by more than 50%.
In cases of prostate enlargement, the combination of both types of medication is more effective in reducing the risk of complications (particularly urinary retention) and lowering the likelihood of surgical intervention.
2. Surgical Treatment
There are several options regarding this type of treatment:
2.1 Classical surgical intervention
It is very rarely used today, being reserved only for certain cases of very large prostate adenomas (150–200 cm³). It involves an abdominal incision and opening of the pelvic cavity, with the complete instrumental removal of the prostate.
It requires a long hospital stay (usually at least 14 days), a prolonged healing time for the abdominal wound, and carries a higher risk of postoperative bleeding.
2.2 Endoscopic interventions
This type of surgical intervention has been in routine use for about 20–25 years and involves the removal of prostate adenoma through a minimally invasive surgical technique, in which an instrument (endoscope, resectoscope) is inserted through a natural pathway of the body (the urethra) to the area compressed by the excess prostatic tissue. The urologist then removes this tissue using various resection methods (high-frequency electric current, laser, or pressurized water vapor).
These treatments are much easier for the patient to tolerate and require significantly shorter hospital stays (5–7 days in the case of resection with electric current or laser, or even just a few hours in the case of water vapor resection).
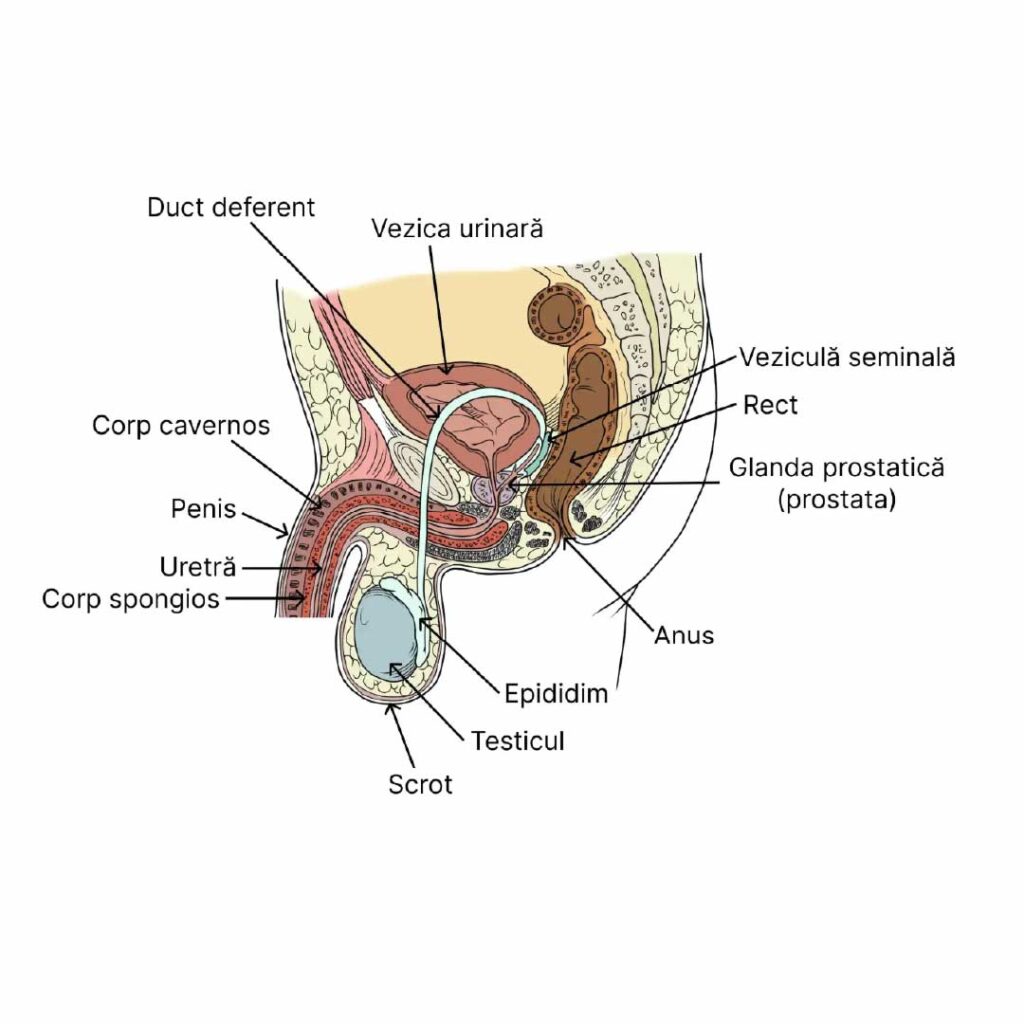
As can be seen in the image, the anatomy of the pelvis and urethra ideally allows minimally invasive endoscopic access (without skin incision) through the natural urinary evacuation channel (the urethra) to the prostate, for the purpose of its removal.
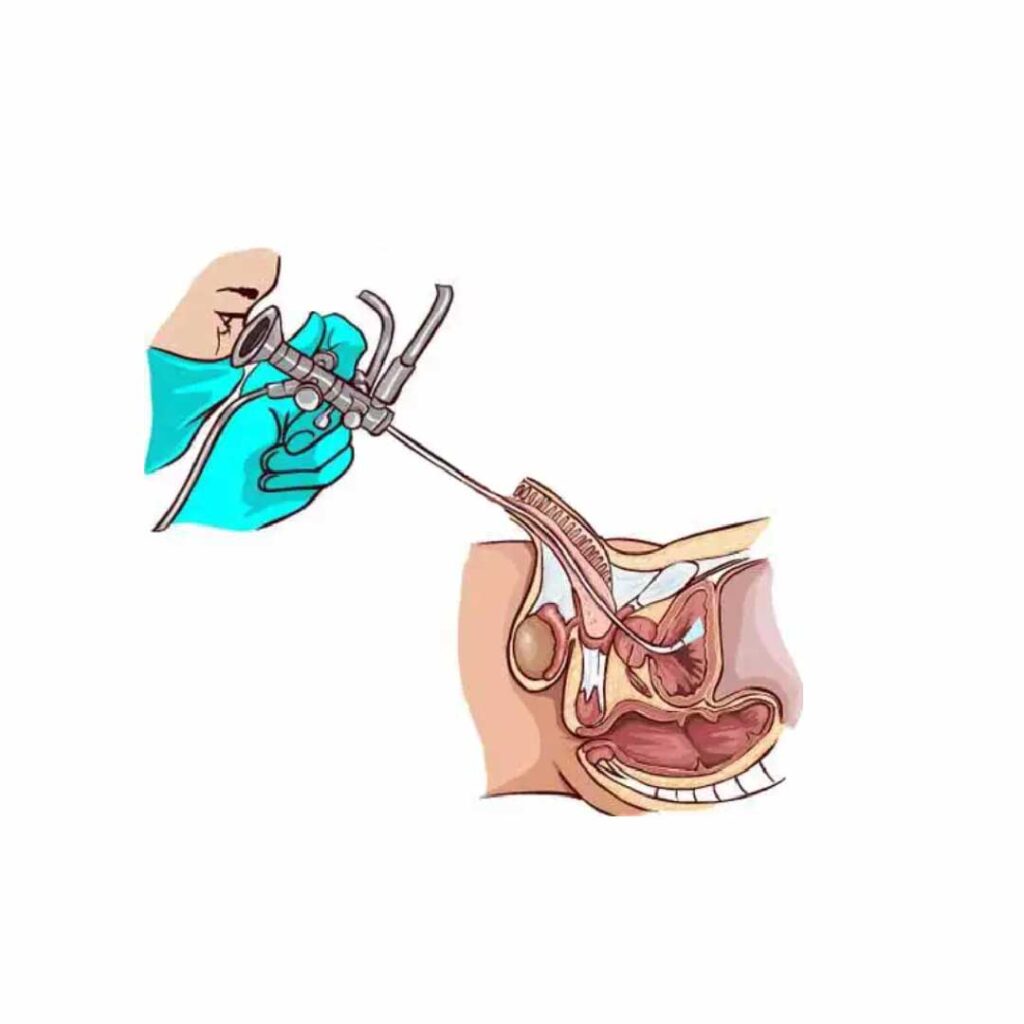
As shown in the image below, by using the endoscopic technique, the urologist has continuous direct optical access to the surgical field (or via a video camera attached to the endoscopic instrument, which transmits the image of the surgical field to a monitor in the operating room).
The main types of endoscopic intervention for prostate adenoma
I. Transurethral resection of the prostate (TURP) – with laser or bipolar electric current, indicated for a prostate volume between 40 and 80–100 cm³.
This medical procedure involves an endoscopic intervention, which requires the insertion of a metal instrument equipped with a video camera. The instrument has a sliding component, represented by a metal loop through which a high-frequency electric current passes, cutting and excising sections of the prostate. The procedure lasts 1–2 hours, is performed under anesthesia (spinal or deep sedation), and requires a hospital stay of 4–10 days, during which the patient undergoes treatment and has a catheter inserted through the urethra to aid the healing process.
It is a surgical method that has been widely used for about 20–25 years.
ADVANTAGES: Rapid improvement in urinary flow, occurring immediately in the postoperative period. Recovery period of approximately 1 month after the procedure.
DISADVANTAGES: – risk of bleeding, during or after surgery; – risk of retrograde ejaculation (when the semen flows back into the bladder and is eliminated through urination instead of ejaculation); – risk of erectile dysfunction.
In the video animation below, you can see how a TURP procedure is performed, as well as how the surgical loop carrying an electric current gradually cuts sections of the prostate, which are then released into the bladder and later removed through irrigation with saline solution via a wide-diameter catheter. The main drawback of this type of intervention can also be observed—namely, the repeated bleeding that inevitably occurs when the electric loop cuts through portions of the prostate. These bleedings are immediately coagulated with the same electric loop, but the risk of bleeding restarting at any time in the immediate postoperative period is quite high, which is why a postoperative hospital stay under strict supervision for 5–7 days is necessary.
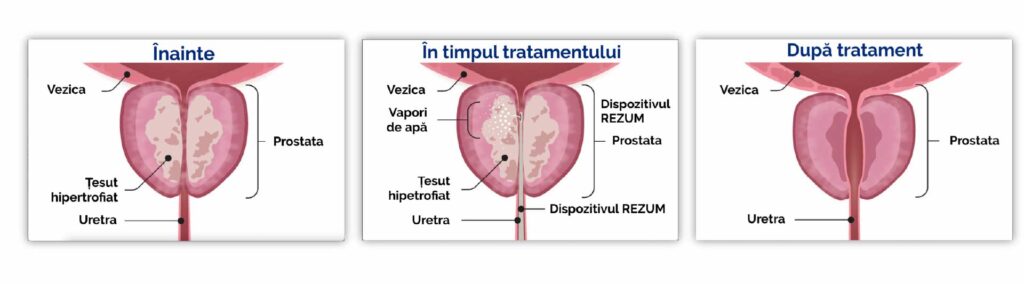
II. Prostate Vaporization Procedure with Steam Vapors
This recently developed medical procedure — performed for the first time in Romania by RO-BOOST Clinic doctors (Dr. Bogdan Gușanu since 2021 and Dr. Emanuel Alexandrescu since 2022, at Med-As Victoria Hospital) — involves an endoscopic intervention similar to the TUR-P technique. It uses a thin needle attached to the end of a specialized instrument, which is inserted into the prostate to perform a series of punctures (4–10), through which pressurized water steam is injected. Once injected, the steam causes a gradual atrophy and eventual disappearance of the prostatic tissue, a process that unfolds over 2–3 months after the intervention. The procedure is minimally invasive, usually requires only local anesthesia or light sedation (the patient is asleep for about 15–20 minutes), and can be performed either on an outpatient basis or in hospital, with a typical hospital stay of up to 12 hours.

ADVANTAGES: – no intraoperative or postoperative bleeding; – no retrograde ejaculation; – no erectile dysfunction; – the procedure can be performed on an outpatient basis or with hospitalization of up to 12 hours; – local anesthesia or sedation.
DISADVANTAGES: – the time period (up to 3 months) required for the prostatic atrophy process to take place.
In the images below, one can observe the considerable widening of the urethral caliber (and thus the improvement of urinary flow) after the procedure, as the prostatic tissue undergoes atrophy.
Technical Considerations on the Prostate Vaporization Procedure Using Steam Vapors
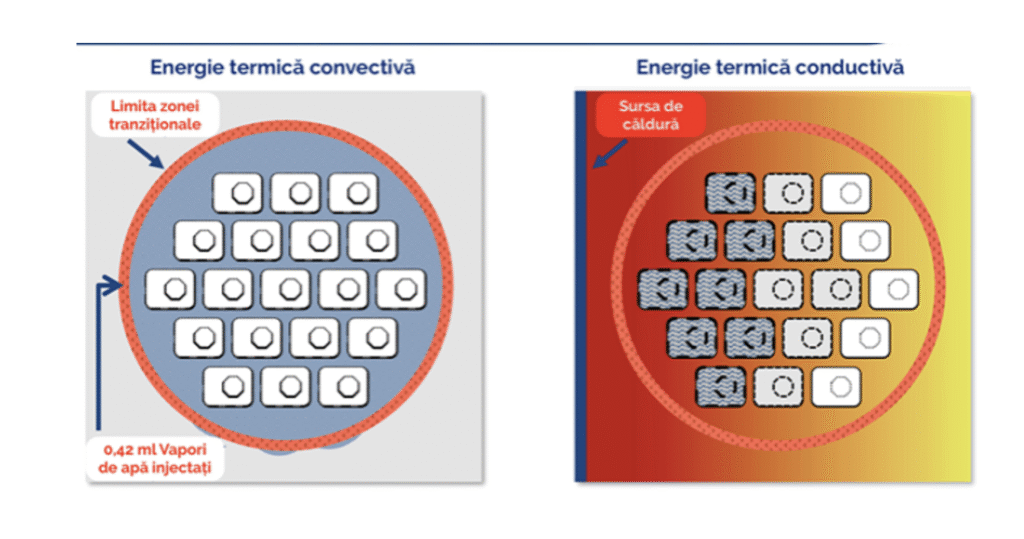
A precise dose of thermal energy from water vapor is delivered into the prostate tissue using a small needle with multiple emission ports, allowing for controlled and even dispersion of the steam. The vapor is administered into the targeted tissue at slightly above interstitial pressure, driving the steam convectively through the tissue spaces, where it condenses and transfers the stored thermal energy directly to the targeted tissue. This convective heat transfer is what distinguishes this procedure from other thermal ablation therapies, which rely on the slower, less precise, and less efficient process of conductive heat transfer.
The convective transfer of thermal energy from the water vapor to the tissue is rapid but also self-limiting. As the water vapor disperses through the tissue, it condenses back into its liquid state, ensuring that the energy does not extend beyond the intended treatment area.
The prostate vaporization procedure with steam is powered by the convective energy of water vapor, delivering targeted and controlled doses of thermal energy stored in the steam directly to the region of the prostate gland — specifically to the tissue responsible for lower urinary tract symptoms secondary to benign prostatic hyperplasia (BPH).
Each 9-second injection treatment uses 0.42 ml of heated sterile water vapor, which rapidly and evenly disperses through the tissue interstices.
The condensation of water vapor releases the stored thermal energy. Cell membranes are denatured, causing immediate cell death, vascularization is sealed, and alpha-adrenergic nerves in the treatment area are denervated, providing an effective, uniform, and predictable treatment.
Over time, this destroyed tissue is reabsorbed through the body’s natural healing response, reducing the volume of tissue, allowing the urethra to open, and relieving lower urinary tract symptoms.
Advantages of the Prostate Vaporization Procedure Using Steam Vapors
In the video below, you can watch the practical execution of a procedure using the prostate vaporization technique. Note the complete absence of any intraoperative bleeding, which gives this method one of its main advantages over the current TUR-P technology.
Frequently Asked Questions
What Does the Prostate Vaporization Procedure Using Steam Vapors Involve?
We perform the procedure under local anesthesia or sedation.
We insert an endoscope through the urethra into the prostate. Using a modern medical device, a visible needle is advanced into the prostatic tissue.
Radiofrequency energy is used to heat water and create steam. The steam is dispersed into the prostate tissue through the needle. We usually repeat this process between two and eight times, depending on the size of your prostate.
The heat from the water vapor travels through the enlarged prostate tissue, causing cell death. In the weeks to months following the procedure, the body reabsorbs the dead cells, leading to a shrinkage of the prostate. This relieves the bladder obstruction that causes urinary symptoms.
What Is the Recovery Process After Prostate Vaporization with Steam Vapors?
You will have a catheter after the procedure. The catheter will drain urine into a bag. The urine bag can be attached to your leg and hidden under your pants. The catheter will be removed in our office seven days after the procedure.
After this procedure, the body triggers an inflammatory response that initially worsens urinary symptoms. For about four weeks following the procedure, it is common to experience burning or stinging during urination. It is also normal to have a slower urine flow, as well as increased urgency and frequency — symptoms that may temporarily be worse than before the procedure.
You may need to take medication to manage your urinary symptoms for about six weeks after the procedure.
You should notice that urinary symptoms gradually improve between four and twelve weeks after the procedure.
Depending on your job, you may be able to return to work about three days after the procedure, although some men prefer to wait until the catheter has been removed.
You will not be able to drive for at least 24 hours after the procedure. Some men prefer not to drive until the catheter has been removed.
What Are the Benefits of the Prostate Vaporization Procedure with Steam Vapors?
The prostate vaporization procedure with steam is an alternative to long-term medication for urinary symptoms caused by benign enlargement of the prostate.
If you are already taking medication for urinary symptoms, in 90% of cases you will be able to stop the medication after the procedure.
The prostate vaporization procedure with steam can be performed as a day surgery — you may go home the same day, provided you are accompanied by a responsible adult.
Some medications and prostate surgeries can cause retrograde ejaculation. Retrograde ejaculation results in a reduced volume of semen during orgasm (a “dry orgasm”). The risk of retrograde ejaculation after the prostate vaporization procedure with steam is approximately 4–6%, which is lower than with many other treatment options.
Some medications and prostate surgeries can cause erectile dysfunction. The risk of erectile dysfunction after the prostate vaporization procedure with steam is very low.
What are the risks
of the Prostate Vaporization Procedure with Steam Vapors?
This procedure is a new surgical technology that had been available only abroad since 2015, and more recently in Romania since 2021.
Currently, there are no studies that have examined the long-term outcomes of the prostate vaporization procedure with steam. It is possible that the benefits of the treatment may decrease over time. For some men, additional treatment for an enlarged prostate may be required in the future.
Improvement in urinary symptoms immediately after the prostate vaporization procedure with steam may not be as rapid as the relief observed with other prostate surgeries, such as transurethral resection of the prostate (TURP) or laser prostatectomy.
As with any surgical procedure, there are potential risks and complications associated with the prostate vaporization procedure with steam:
Bleeding: The risk of blood loss is minimal. The risk of bleeding requiring a blood transfusion is ≤1%.
Infection: ≤5%. Broad-spectrum antibiotics are administered at the beginning of the procedure to minimize the risk of a urinary infection.
Retrograde ejaculation: ≤2%
Erectile dysfunction: ≤2%.
What Are the Possible Immediate Side Effects
After the Prostate Vaporization Procedure with Steam Vapors?
Temporary burning and stinging when urinating (which may last 5–7 days) | 1 in 3 patients (33%) |
Temporary blood in the urine (which may last 5–7 days) | 1 in 4 patients (25%) |
Temporary pain or discomfort in the pelvic area | Between 1 in 5 and 1 in 6 patients (16–20%) |
Urinary tract infection requiring antibiotic treatment | 1 in 15 patients (6–7%) |
The procedure may not relieve all of your symptoms, and you may need additional treatment within 4 years. | 1 in 25 patients (approximately 4%) |
Procedura de vaporizare prostatica cu vapori de aburi este o opțiune pentru dvs. dacă:
You do not want to take, or cannot take, medication for an enlarged prostate.
You do not want to undergo a more invasive procedure, such as transurethral resection of the prostate (TURP) or laser prostatectomy.
You do not want a prolonged hospitalization of 5–7 days, with inherent risks of bleeding/infection and subsequent impact on sexual life.
Your prostate is between 30 and 120 grams. (A normally sized prostate is less than 25 grams.)
You prefer to preserve erectile and ejaculatory function, maintaining a normal sexual life after treatment.